



AI-Driven Digital Stewardship System to Reduce Irrational Antibiotic Dispensing in Community Pharmacies
Bangladesh
Healthcare
Implementing Organisation
CMED Health Limited
Bangladesh, Bangladesh, Dhaka
Implementing Point of Contact
Md Jobayer Rahman
Research Associate, AIMS Lab, Institute of Research, Innovation, Incubation & Commercialization (IRIIC), United International University (UIU)
Contributor of the Impact Story
World Health Organization (WHO)
Year of implementation
2023
Problem statement
Antimicrobial Resistance (AMR) in Bangladesh is accelerating due to widespread irrational antibiotic dispensing, self-medication, and lack of prescription verification systems. AMR rates have increased by 11% over five years, with some antibiotics losing up to 82% effectiveness ommunity pharmacies often function as primary healthcare access points, yet lack digital tools to verify prescriptions, audit dispensing behavior, or track patient history. Financial barriers to physician consultations further drive symptom-based antibiotic purchases. The absence of integrated digital health accounts prevents longitudinal monitoring of antibiotic adherence. This use case addresses the structural governance gap in antibiotic stewardship by deploying an AI-enabled digital ecosystem that enforces prescription verification, triages high-risk patients to telemedicine, and monitors dispensing patterns in real time.
Submission Overview
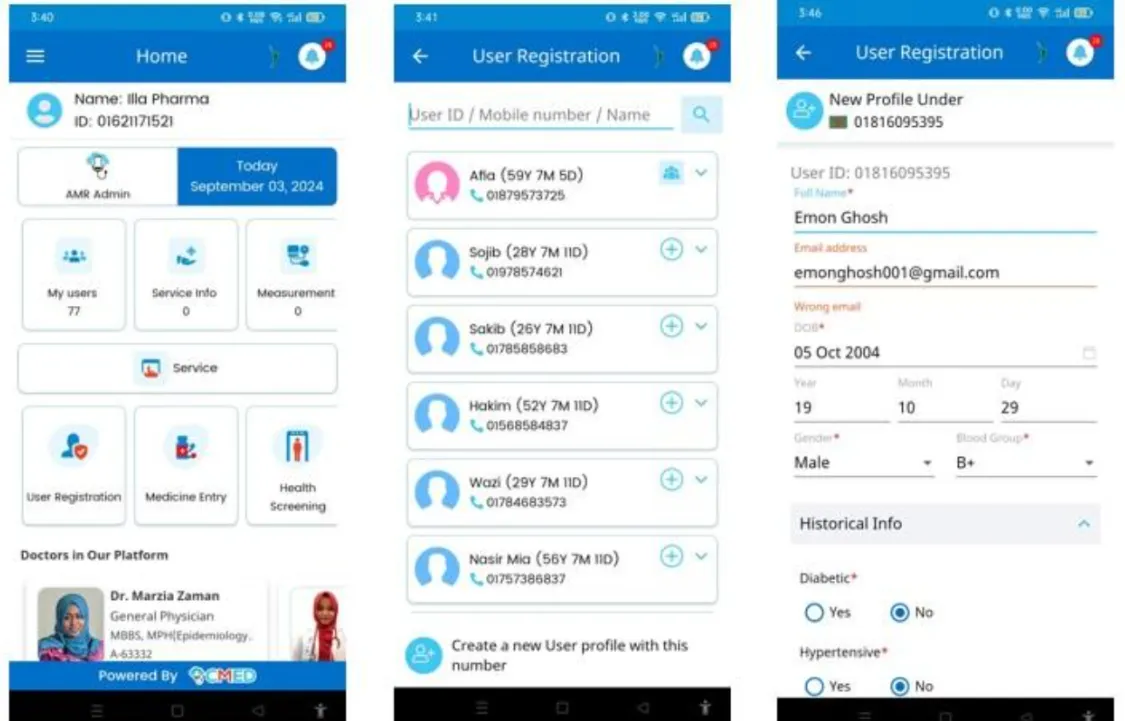
CMED Health Limited is a Bangladesh-based digital health technology company focused on integrating AI-driven clinical decision support systems into primary healthcare settings. In collaboration with the Advanced Intelligent Multidisciplinary Systems (AIMS) Lab at United International University and Bangladesh Medical University (BMU), CMED develops scalable digital health ecosystems designed to improve access, quality, and governance in low- and middle-income healthcare environments. The organization specializes in AI-powered triage systems, telemedicine integration, pharmacy digitization, and public health surveillance dashboards. Its work focuses on addressing structural healthcare gaps, including irrational antibiotic use, lack of digital medical records, and limited access to licensed physicians in retail pharmacy settings.
AI Technology Used
Key Outcomes
Accuracy & Quality Improvement
Access & Reach
Resilience & Risk Reduction
Inclusion & Equity
Resource Efficiency
CMED Health Limited’s AI-Driven Digital Stewardship System demonstrates measurable improvements in antimicrobial governance within urban community pharmacies in Dhaka. Over a three-month pilot across 28 pharmacies serving 2,654 users, the intervention significantly increased prescription-guided purchases (from 27.59% to 43.49%) while sharply reducing symptom-based, unverified medicine purchases (from 18.84% to 6.42%). High-risk antibiotic dispensing without prescription fell from 4.05% to 0.86%, and antibiotics as a share of total medicine sales declined from 23.05% to 17.90%. By embedding AI triage, telemedicine referral, and real-time dispensing oversight into pharmacy workflows, the model addresses structural drivers of irrational antibiotic use and establishes a scalable digital governance framework for antimicrobial resistance mitigation in low- and middle-income settings.
Impact Metrics
Increase in medicines dispensed with a valid physician prescription due to AI triage and telemedicine integration
Baseline Value
Before implementation, only about 27.59% purchases were supported by a verified prescription, reflecting heavy reliance on informal OTC access Percentage of total purchases
Post-Implementation
After AI-enabled triage and mandatory telemedicine referral for high-risk cases, nearly 43.49% purchases were prescription-guided Percentage of total purchases
Reduction in medicine purchases made solely on the basis of self-reported symptoms following AI-enabled screening and point-of-sale workflow controls
Baseline Value
Before implementation, 18.84% of purchases were symptom-based and unverified, indicating weak antimicrobial stewardship at pharmacy level Percentage of total purchases
Post-Implementation
After AI triage and transaction monitoring were introduced, symptom-only purchases declined to 6.42% Percentage of total purchases
Reduction in antibiotics dispensed without prescription in symptom-based cases due to AI gatekeeping and mandatory telemedicine referral
Baseline Value
Prior to implementation, 4.05% of total purchases involved antibiotics sold purely based on symptoms without prescription validation Percentage of total purchases
Post-Implementation
Following AI enforcement controls, this high-risk dispensing behavior decreased to 0.86% Percentage of total purchases
Reduction in antibiotics as a share of overall medicine sales due to AI-supported prescription verification and dispensing oversight
Baseline Value
Before implementation, antibiotics accounted for 23.05% of total medicines sold, reflecting overuse in comm After digital stewardship mechanisms were introduced, antibiotics comprised 17.90% of total medicine volume Unit: Percentage of total medicine volume
Post-Implementation
After digital stewardship mechanisms were introduced, antibiotics comprised 17.90% of total medicine volume After digital stewardship mechanisms were introduced, antibiotics comprised 17.90% of total medicine volume Unit: Percentage of total medicine volume
Implementation Context
28 community pharmacies across two selected areas of Dhaka, Bangladesh
2,654 unique pharmacy users from urban, low-and middle-income populations, patients seeking OTC antibiotics, community pharmacy customers
Key Partnerships
CMED Health Limited, United International University (AIMS Lab), Bangladesh Medical University, and community pharmacies
Replicability & Adaptation
- Align economic incentives for pharmacy sellers to reduce resistance
- Simplify patient onboarding to improve data completeness
- Integrate with national digital health ID systems where available
- Customize triage models to local epidemiology
- Ensure regulatory alignment for digital prescription validation
The model can be replicated in other LMIC urban pharmacy networks but requires contextual adaptation to regulatory environments, pharmacy incentive structures, and digital infrastructure.
Supporting Materials

* The data presented is self-reported by the respective organisations. Readers should consult the original sources for further details.